Kava Safety Confirmed - No Liver Damage: Tackling the 8 reported factors that have allegedly been identified as potential causes of liver injury from kava use.
Addressing Factors Routinely Identified in Literature

Misidentification of cultivar variation
In the quest to understand the liver toxicity concerns associated with kava, various hypotheses have been proposed. One such hypothesis is the "misidentification of cultivar preparation," which suggests that different cultivars of the kava plant contain varying levels of toxic constituents. However, a study by Lechtenberg et al. (2008) titled "Is the Alkaloid Pipermethystine Connected with the Claimed Liver Toxicity of Kava Products?" published in Die Pharmazie found that pipermethystine in concentration levels of 10 mg/kg is not toxic in any animal models. This is far above the levels that could be consumed even with non-noble extracts. This study scrutinizes the role of pipermethystine in liver toxicity and concludes that it is not a contributing factor. This finding challenges the notion that pipermethystine levels in different parts of the plant could be responsible for the liver issues reported in the late 90s and early 2000s. Flavokavain B was also thought to be part of this issue; however, further studies into the toxicity of this compound found again that there would again be no way to reach levels thought needed to reach liver toxicity, and would require 250 times the average FKB consumption seen (Teschke et al. 2011).
Use of inappropriate plant parts
In the same vein as number 1, this assertion of “inappropriate plant parts” is based upon the hypothesis that pipermethystine, the alkaloid found in the upper portion of the plant, is toxic, and based on the current research, this is not the case.
Adulteration and contamination of kava products
This was a hotly debated area between 1998 and 2003. Here we see the cluster of adverse event reports allegedly related to kava. Inadvertent contamination of the supply could be due to fungal/mold hepatotoxins. Teschke et al. (2011) mentioned concerns regarding fungal contamination in relation to liver injury from kava use. It states that kava raw material, particularly the peeling of roots and rhizomes, can be contaminated by mold hepatotoxins such as aflatoxins after harvest and during storage. There is evidence that kava roots are naturally contaminated with aflatoxins, which are compounds toxic to the human liver. Other fungi with similar hepatotoxicity potency are also considered potential candidates. The quantity of fungi present is an important factor in the possible hepatotoxicity of an array of products. The bark of kava rhizomes and roots may contain higher numbers of bacteria and fungi, which could contribute to higher levels of mycotoxins. Note that we have not seen reported hepatotoxicity-related events for at least 20 years since the rash reported in the late 1990s to early 2000s.
Prolonged treatment duration
Here, we run into the realm of personal and “professional” opinions. Epidemiological data suggest that kava has been consumed for millennia without health issues (Singh 2004). There is no upper limit of “treatment duration” in which there is a sudden increase in liver-related issues. In fact, if we go back and look at the old documentation from BfArM (essentially the German FDA), we can see that all of these instances had widely ranging time frames, from 1 month to over 1 year (Teschke et al. 2003). These cases were thrown out in 2015 and are not to be viewed as causative by kava (Kuchta et al. 2015).
Daily overdose of kavalactones
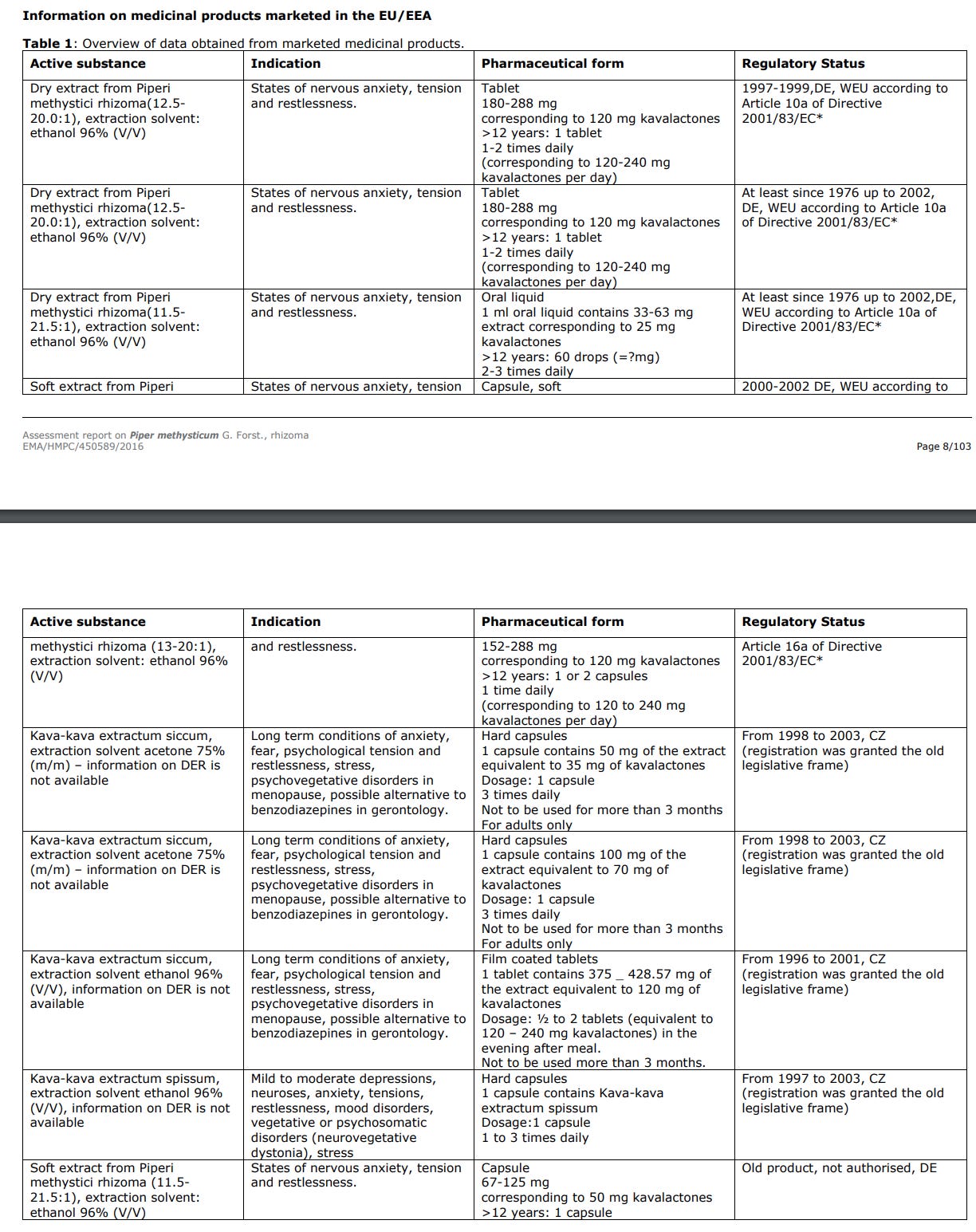
Again, this is purely subjective, and each researcher or subcommittee has their own suggestion as to what constitutes a “daily dose”. There is no safety guideline at which this is suggested, only efficacy seen in reduction in situational stress and anxiety. We technically have no upper limit of dose for what is “suggested”. Table 1 outlines the various recommendation data marketed by manufacturers in the EU/EEA (HMPC 2017).
Comedication with other herbs, dietary supplements, or synthetic drugs
This area should not go unaddressed simply because it is mentioned so often. Currently, there is no research suggesting that any drugs consumed could be made further toxic with the inclusion of kavalactones at human concentrations. Any research that suggests this toxicity has used concentration levels of either the kavalactones or the toxic compound in question at quantities not seen in any type of human consumption. Essentially, researchers increased the levels of both kavalactone and toxic components until toxicities were observed without any respect to the concentration levels seen in humans at specific organs in typical scenarios. One area where bloggers and article writers love to cite is specific drugs that they say can cause pharmacokinetic interactions when consumed with kava. These suggestions are based solely on adverse event reports. When we open the front page of the Federal Adverse Event Reporting System (FAERS), we encounter several disclaimers. One being: “Existence of a report does not establish causation”. It seems fundamentally that these authors have forgotten that simply because adverse event reports appear, this does not necessarily mean they are correlated to kava in any way.
Alcohol use
This is a touchy subject where opinions abound, but we must look at the research provided instead of making hasty assumptions. There are several studies on kava and alcohol. We now look at the most recent study by Abdulabbas et al. (2022). In this study, the researchers increased the levels of kavalactones to 800 mg/kg and applied this to rats with a blood alcohol content of 5% to identify any type of toxicity. As you can see, these researchers are attempting to state that the combination is dangerous; however, again, these dosages of both kavalactones and ethanol are rather impossible for any human to achieve. Be that as it may, alcohol is a known liver toxin, and the combination of long-term consumption of alcohol and kava would cause no more liver issues than alcohol consumed alone. Kavalactones have also been shown not to interact with alcohol dehydrogenase (Anke et al. 2006). It should be well understood that although we do not have convincing evidence that kava and alcohol are toxic to the liver, we do not have subsequent research regarding other organs that may be affected. The suggestion remains to avoid this combination.
Preexisting liver disease
No research has suggested preexisting liver disease as a comorbidity in kava consumption. In fact, there has been no research involving the application of kava in a stressed liver. If liver disease exists, it is a preexisting condition.
In summary, the eight commonly cited factors implicated in liver injury due to kava use warrant nuanced examination based on existing scientific literature. Misidentification of cultivar variation and use of inappropriate plant parts have been largely debunked as contributing factors, given that pipermethystine, once thought to be toxic, has been found non-toxic at levels far exceeding human consumption. Adulteration and contamination, particularly with mold hepatotoxins such as aflatoxins, remain a plausible concern, although no new hepatotoxicity-related events have been reported in the past two decades. Prolonged treatment duration and daily overdose of kavalactones lack empirical evidence to substantiate liver toxicity claims. Co-medication with other substances and alcohol use have been studied, but the research often employs unrealistic concentration levels, making the findings less applicable to human scenarios. Lastly, preexisting liver disease has not been studied in relation to comorbidity in kava consumption. Overall, while caution is advisable, especially in the context of adulteration and contamination, many of the traditionally cited factors for liver injury related to kava use are not supported by rigorous scientific evidence.
Sources:
Anke, J., S. Fu, and I. Ramzan. 2006. “Kavalactones Fail to Inhibit Alcohol Dehydrogenase in Vitro.” Phytomedicine: International Journal of Phytotherapy and Phytopharmacology 13 (3): 192–95. https://doi.org/10.1016/j.phymed.2004.07.005.
Abdulabbas Hasan, Mohammed, Syam Mohan, Heshu Sulaiman Rahman, Hemn Hasan Othman, Shirwan Hamasalih Omer, and Abdullah Farasani. 2022. “The Sub-Acute Toxicity of Kavalactone in Rats: A Study of the Effect of Oral Doses and the Mechanism of Toxicity in Combination with Ethanol.” Drug and Chemical Toxicology, May, 1–9. https://doi.org/10.1080/01480545.2022.2069803.
Committee on Herbal Medicinal Products (HMPC). 2018. “Assessment Report on Piper Methysticum G. Forst., Rhizoma.” European Medicines Agency. https://www.ema.europa.eu/en/documents/herbal-report/final-assessment-report-piper-methysticum-g-forst-rhizoma_en.pdf
Kuchta, Kenny, Mathias Schmidt, and Adolf Nahrstedt. 2015. “German Kava Ban Lifted by Court: The Alleged Hepatotoxicity of Kava (Piper Methysticum) as a Case of Ill-Defined Herbal Drug Identity, Lacking Quality Control, and Misguided Regulatory Politics.” Planta Medica 81 (18): 1647–53. https://doi.org/10.1055/s-0035-1558295.
Lechtenberg, M., B. Quandt, M. Schmidt, and A. Nahrstedt. 2008. “Is the Alkaloid Pipermethystine Connected with the Claimed Liver Toxicity of Kava Products?” Die Pharmazie 63 (1): 71–74. https://www.ncbi.nlm.nih.gov/pubmed/18271308.
Research, Center for Drug Evaluation And. “FDA Adverse Event Reporting System (FAERS) Public Dashboard.” U.S. Food And Drug Administration, October 22, 2021. https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard.
Singh, Yadhu N. 2004. Kava: From Ethnology to Pharmacology (Medicinal and Aromatic Plants - Industrial Profiles). CRC Press.
Teschke, Rolf, Samuel X. Qiu, and Vincent Lebot. 2011. “Herbal Hepatotoxicity by Kava: Update on Pipermethystine, Flavokavain B, and Mould Hepatotoxins as Primarily Assumed Culprits.” Digestive and Liver Disease: Official Journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver 43 (9): 676–81. https://doi.org/10.1016/j.dld.2011.01.018.
Teschke, R., W. Gaus, and D. Loew. 2003. “Kava Extracts: Safety and Risks Including Rare Hepatotoxicity.” Phytomedicine: International Journal of Phytotherapy and Phytopharmacology 10 (5): 440–46. https://doi.org/10.1078/0944-7113-00314.